I recognize weight loss and diet are sensitive topics in the Lipedema Community. Skip this one if it’s a trigger for you.
Also, this isn’t a recommendation for you, so talk with your doctor if you haven’t already. This is just what I’ve learned and where I personally am at this morning. OK, caveats over…
Hi friends,
Well, wow, what timing!
This week I had the opportunity to hear one of the doctors on the Lipedema Education Group give a presentation to the team about the injectable GLP-1 agonist drugs (Ozempic), and GLP-1 and GIP receptor agonist drug (Mounjaro) being used for diabetes, and some for obesity. He went into a lot of detail about what he’s seen as a physician and a lot of the research studies that he has reviewed and teaches from. He also took the time to explain to the non-medical folks on the call, what GLP-1s and GIPs are, how they work in layman’s terms which was great. Unfortunately, I cannot share his presentation as it was used in a different conference, (and they get kind of strict about slide sharing). And of course, without his actual dialogue the slides would be really hard to understand anyway. But this doctor’s presentation helped me to understand the differences between the drug types. The timing of his sharing is perfect. Because on the news yesterday, we got word that the FDA has finally approved tirzepatide, the same drug as Mounjaro, for weight loss, under the brand name Zepbound. See their press release here.

While I believe in loving yourself as you are and not beating myself up over diets anymore, and definitely not letting myself feel guilty for what I eat (and I don’t), I would personally like to lose some non-lipedema weight for a couple of actual medical reasons: I need my knees replaced due to hypermobility and bone on bone arthritis. These old knees hurt most nights and dislocate and lock up unpredictably. While my orthopedic surgeon will do the surgery to replace the knees when I tell him it’s time (and not based on weight), we have discussed having better outcomes on knee replacement as a 50-year-old with less weight. Also, I need some serious work on my lymph nodes behind my left knee to try and help lymphedema, and I’m 75 lbs. over the weight limit (there’s an actual medical reason for this – lymphatics are so very delicate and cannot have extra pressure from adipose tissue on them to take the repair, so I get it, but I don’t love it). So, I need to really see if I can drop that 75 lbs. But I also need to stop weight cycling (ya know, where you lose weight, gain it back, lose weight, gain more) because it is SO hard on the body. Severe weight cycling (aka ME) is associated with a more than fivefold risk of sarcopenia, which mean loss of muscle mass and strength.
Long ago, when my second bariatric surgery (lap band, again), failed and blew out my esophagus, I vowed for myself personally, no more keto. I’d been incredibly, 100% compliant with keto for an entire year and lost well over 100 lbs. I hated keto, I was miserable and I felt left out of all the good food fun. And the second I strayed from it, BOOM, all of the weight I’d lost came back, along with all that guilt and blah blah blah. The problem is, the burden of this diet is too much for my busy lifestyle and preferences. I’m not a food prepper and I never will be. It’s not sustainable nor frankly, enjoyable for me, Susan O’Hara. For those of you who follow keto and do great on it, yay! It’s just not for me, so please don’t blast me in the comments. I get it. I also vowed that life was way too short to totally eliminate foods that I really enjoyed. Food gives me joy and I’m not afraid to say it. Yes. I do like food. How about you? Anyway, I digress…

If you’ve followed me for very long, you’ll remember that I ‘just’ posted about findings about these drugs presented at the Lipedema World Congress, in a post located here. The general conclusion of the presentation was that if you use the drugs, they don’t replace conservative or aggressive lipedema therapies and shouldn’t delay surgical treatment. The drugs helped lipedema patients adhere to lipedema-specific diets, and they had anti-inflammatory properties, so the presentation was good and supported what I learned the other day. However it was required to be a short presentation and left out a lot of the science.
And remember Ozempic/Wegovy/Semaglutide already had an approval for weight loss under a different name than the brand for diabetes only, but it’s Mounjaro a lot of us who have obesity on top of lipedema have been waiting for. The reason Mounjaro interests me is that it actually has two actions where the Ozempic only has the one. Mounjaro/tirzepatide acts on two receptors in the body, while Ozempic/semaglutide only acts on the GLP-1 agonist receptor. Here is a comparison article about the two drugs from DrugWatch.com, if you’re into more of the medical side of things.
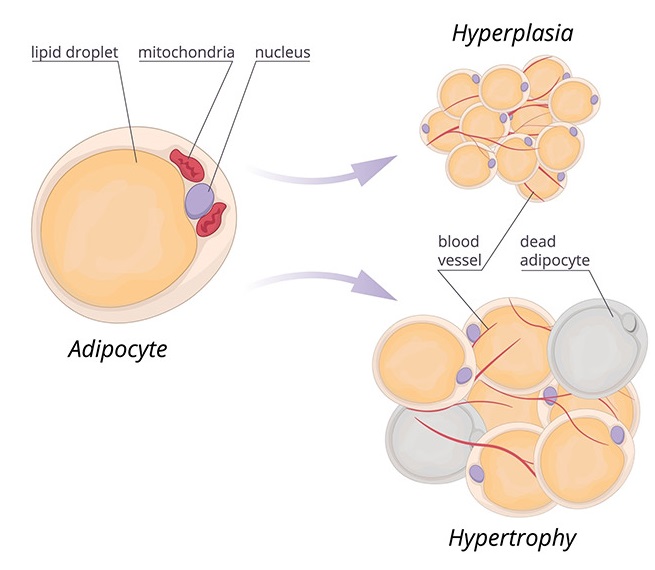
Adding in the ability to affect two receptors instead of one is kind of a big deal. Tirzepatide/Mounjaro/Zepbound has the effect on the Glucose-Dependent Insulinotropic Polypeptide Receptor Agonist (GIP – say that twice!) where Ozempic doesn’t. What’s this mean? This drug works on how fat is stored in your body when you have excess nutrition to be stored. It changes from making existing fat cells bigger (hypertrophy), which causes the cell to act all crazy and become inflamed and be less sensitive to insulin, to adding new fat cells (hyperplasia) instead. Also, having bigger fat cell size relative to the overall size of fat depots is a strong risk factor in the future development of type 2 diabetes, so we want to have more, but smaller fat cells instead of existing fat cells getting larger. When we eat more than we need and make new fat cells instead of growing our existing cells bigger, the new ones aren’t diseased and inflamed, and they are also still sensitive to insulin, and that’s a good thing. So having that GIP receptor agonist makes our fat function like it’s supposed to instead of making our fat sicker. It’s really complicated and I’m only touching on what the science says.
What I know after my recent learning is that if I can switch to tirzepatide, I’m going to because of the way it helps manage fat cell health. If you’re like me, and just not into dedicating your whole life and mindset to weight loss, why not get all the help we can? This drug may be an absolute game changer for those of us with lipedema and who struggle to get our non-lipedema fat gone. For reference, here is a link to their approved package labelling from the FDA, released November 8, 2023.
For me, I’ve been on Ozempic for a while now. I was on Mounjaro during the three months’ time their $25 coupon worked, but since I’m not diabetic, my pricing was going to be over $1000 a month, which is not sustainable for a retiree like me. So I’ve been on Ozempic for around $23 a month. Sadly, I’d say the last two weeks since I titrated up to a higher dose are the first times I’ve felt its effects with the food chatter in my head finally slowing down, so I actually haven’t lost any weight. I’m excited to try the Mounjaro again with a longer term plan, knowing more about the science now too. I’ve already emailed my doctor this morning to see if she will help me make the switch to ZepBound, but not let me go without the Ozempic while the pharmacy gets their first shipment in. I still plan to swim at least 3-4 times a week, and continue to add good foods like good proteins, fruits and veggies to what I eat. (Oh yeah, I took on the mindset of adding stuff to what I eat instead of taking things away. It makes me way happier. It’s hard. All of it.) And now that I’ve learned about Sarcopenia, my plan is to head to the YMCA down the street a couple of times a week for some strength training to see if I can help make myself stronger.
What Happens When I hit Goal Weight? Do they make me get off the drug?
We’ve all heard that you gain the weight you lost, back after stopping these drugs (I don’t have data links to support this), so it would be an absolute travesty to not stay on the meds once you hit goal weight. Well Eli Lilly thought about that. The package insert indicates a maintenance dose of 5 mg weekly. From the package insert, “The recommended maintenance dosages of ZEPBOUND in adults are 5 mg, 10 mg, or 15 mg injected subcutaneously once weekly. Consider treatment response and tolerability when selecting the maintenance dosage. If patients do not tolerate a maintenance dosage, consider a lower maintenance dosage.” Of course insurance approving the maintenance dose is another story, but this is what’s recommended, so keep this info handy when it comes time to fight insurance on covering your maintenance dose.
Should YOU Take Ozempic or Mounjaro? (Directly quoted from DrugWatch.com)
“Whether you should take Ozempic or Mounjaro depends on your individual treatment needs. Mounjaro is more effective for weight loss and lowering A1C, but it could also come with a greater risk of side effects — particularly severe gastrointestinal side effects.
Ozempic is effective at lowering A1C and helping people lose weight, but it’s also FDA-approved to prevent cardiovascular events in people with established cardiovascular disease. People with Type 2 diabetes already have an increased risk of these health problems. Using Ozempic could help lower the risk of serious heart attack, stroke or even death.
Before making a choice on which drug to take, make sure to talk with your health care providers about the pros and cons of each medication. It’s possible to switch from one drug to the other if your results aren’t optimal with the first drug you take.”
That was long! What are your thoughts now that Zepbound is here?
As usual, hang in their friends. Diet and weight loss is complicated and comes with so much emotional baggage. Let’s do the best we can but remember to enjoy life every single second! Also as usual, I hope this information helps someone, just one more person.
Susan
Resources
Longo, Michele, Federica Zatterale, Jamal Naderi, Luca Parrillo, Pietro Formisano, Gregory Alexander Raciti, Francesco Beguinot, and Claudia Miele. 2019. “Adipose Tissue Dysfunction as Determinant of Obesity-Associated Metabolic Complications” International Journal of Molecular Sciences 20, no. 9: 2358. https://doi.org/10.3390/ijms20092358
Lundbäck V, Kulyté A, Arner P, Strawbridge RJ, Dahlman I. Genome-Wide Association Study of Diabetogenic Adipose Morphology in the GENetics of Adipocyte Lipolysis (GENiAL) Cohort. Cells. 2020 Apr 27;9(5):1085. doi: 10.3390/cells9051085. PMID: 32349335; PMCID: PMC7291295.